
In this article, you'll learn
What is Bowel Obstruction
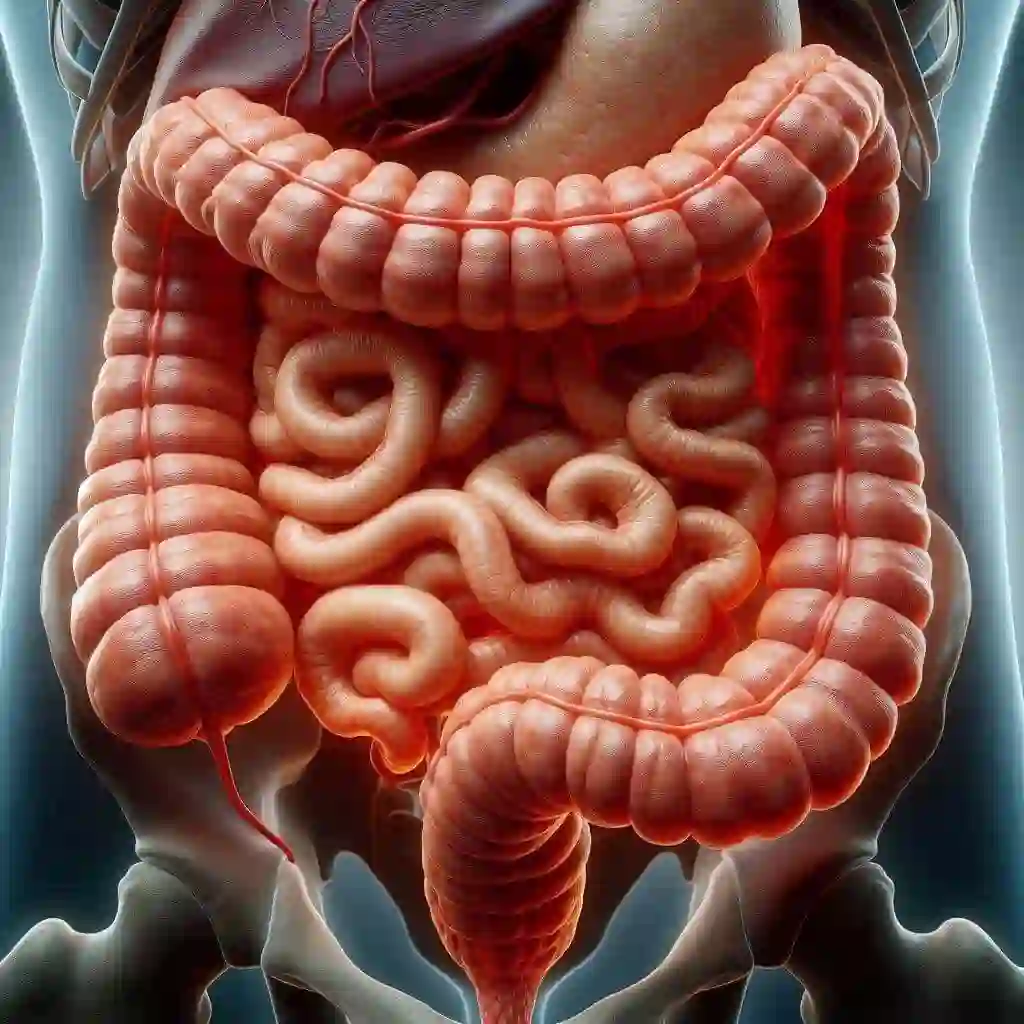
A bowel obstruction occurs when the lumen of the bowel (small or large intestines) becomes blocked either partially or completely. It can be mechanical (physical blockage of the intestines inhibiting intestinal contents) or functional (pseudo-obstruction) blockage (when the content of the lumen is not moving to free the intestine or intestinal peristalsis becomes difficult. Typical example is paralytic ileus and Hirschsprung's disease). The bowels serve as passage way for food waste to be eliminate from the body. When this passage way is obstructed by any means (such as twisting of the intestines, adhesions, the intestines telescoping into itself, scarring), prevents the normal peristalsis of digested products leading to a serious complication if attention is not given. Hence bowel obstructions are serious medical emergency which require immediate intervention
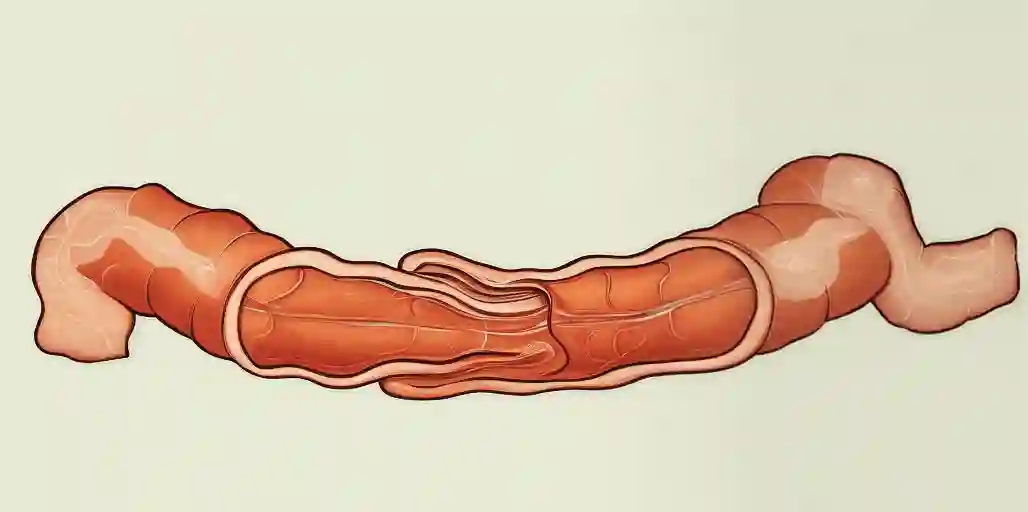
Intestinal telescoping
Large Bowel Obstruction (LBO)
Large bowel obstruction is interruption of part or all of the large intestine. As a result, waste remains in the body which requires treatment to ease problems and complications. Prolong obstruction can result in tissue death and bursting of the intestines and as a result, death which is a serious complication. Majority of the obstruction occurs at the distal or distal to transverse colon. It accounts for twenty percent of all intestinal obstruction and SBO far the commonest. It can also be partial or complete obstruction.
Small Bowel Obstruction (SBO)
SBO refers to the mechanical interruption of the patency of the intraluminal tract of the small intestine resulting in difficulty peristaltic function. It is more common than LBOs which requires immediate surgical intervention. It is usually caused by scar tissue, hernia, or cancer. SBOs can occur as strangulated (indicates that blood flow is compromised, and may lead to intestinal ischemia, necrosis, and perforation which requires surgical intervention) or Non-strangulated (also known as simple obstruction, which can be managed conservatively), partial or complete obstruction. It can be classified as functional or mechanical. Strangulation is the most severe complication of small bowel obstruction. SBOs present with abdominal distention, pain, nausea and vomiting, constipation or obstipation (severe form of constipation, this ability to pass gas or hard stool).
Incidence
Bowel obstructions affects both males and females equally by small and major intestinal blockages. Small bowel obstructions (SBOs) are more common than large bowel obstructions (LBOs) and are the most frequent indication for surgery on the small intestines. Previous abdominal surgery and conditions such as, colon or metastatic cancer, chronic intestine inflammatory disease, current abdominal wall, and/or an inguinal hernia, and foreign body ingestion are all factors that influence the incidence intestinal bowel obstruction. SBO causes about 80% of all bowel obstructions
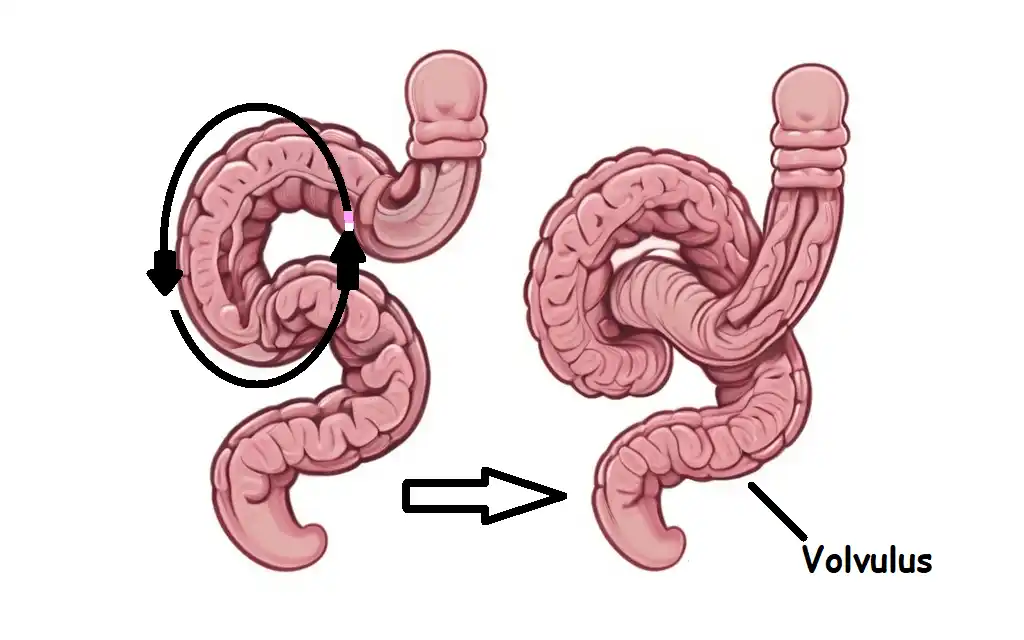
Twisting of the bowel around itself
Causes of Bowel Obstruction
There are several potential causes of bowel (small and large) obstructions which includes but not limited to the following
- Twisting of the bowel around itself (volvulus)
- A stricture of the bowel caused by scar tissue from conditions, such as diverticulitis and Crohn’s disease
- Sliding or telescoping of a part of the bowel into another part (intussusception)
- Impaction of foreign bodies within the bowel lumen
- General anesthesia
- Adhesions
- certain pain relief medications
- Impacted feaces (hard lump of stool)
- Incarcerated hernia
- IBD or abscess
- Bowel cancers
- Nerve and muscle disorders such as Parkinson’s disease, Hirschsprung’s disease
You may also like: Pathophysiology of Intussusception
Risk factors of Bowel Obstruction
The following events and conditions can increase one risk of getting bowel obstruction occurring:
- Adhesion from previous abdominal or pelvic surgery
- cancer, especially in the abdomen
- Crohn's disease, which thickens the intestinal wall
- Ulcerative colitis
- Radiation therapy
Types of bowel obstructions
Complete obstructions:this is severe form of bowel obstruction where part or the entirely bowel is blocked. This prevent all peristaltic activities including, solids, liquids, and gases from the lumen of the lower digestive tract. There is difficult passing stool or gas, thus constipation or obstipation. Complete bowel obstruction has a higher failure rate with conservative therapy, thus, a life-threatening emergency that require emergency treatment or surgery.
Partial obstructions:A less severe form of intestinal obstruction. These are interruption of some part, but not all, of the intestine is blocked. There is observed slow movement of solids, liquids, and gases through the digestive tract. A partial bowel obstruction may cause discomfort, bloating, and diarrhea.
Closed-loop obstruction:A closed-loop obstruction refers to a type of obstruction in the small or large bowel in which there is complete obstruction distally and proximally in the given segment of the intestine.
Pseudo-obstruction:A pseudo-obstruction is when there are symptoms of bowel obstructions but actual blockage is not present. It occurs as a result of intestinal muscle or nerve damage which prevent the normal movement of solid, liquids, and gas through the intestines. It is a rare condition that manifest as intestinal bowel obstruction. Conditions such paralytic ileus and Hirschsprung's disease can cause Pseudo-obstruction as well as other activities as opioid drug use.
Pathophysiology of Bowel Obstruction
The normal physiology of the bowel consists of the digestion of food and the absorption of nutrients, vitamin synthesis, water absorption, and bilirubin breakdown. Once the bowel has done its work and absorbed all essential nutrients from food, the waste travels to the rectum and pass out as feces. Intestinal obstruction can be classified into small bowel and large bowel obstruction. The large bowel (also known as the colon, or large intestine), begins at the final portion of the small bowel (small intestine) and continue all the way to the rectum.
When the bowel is obstructed or the rectum leads to significant dilatation of the bowel proximal to the obstruction, intraluminal pressure increases, which leads to cascade of events such as compromising intestinal venous outflow resulting in edema, reducing arterial blood flow in bowel wall resulting in ischemia. As a result, there is an increase bacterial translocation, systemic inflammatory response syndrome (SIRS), dehydration and electrolyte abnormalities due to mucosal permeability of the colon. As the bowel wall becomes edematous, it shortens in length, loses its mucosal integrity, contributing to fluid loss and diminished absorptive capacity. Fluid loss from emesis, bowel edema, and diminished absorptive capacity leads to dehydration. Eventually, ischemia, necrosis, and perforation results in generalized peritonitis, multi-organ failure and potentially death.
Signs & Symptoms of Bowel Obstruction
- Abdominal distention and bloating
- Nausea and vomiting
- Diarrhea
- Malaise
- Fever
- Loss of appetite
- Colicky cramp-like abdominal pain
- straining at stools
- constipation and or obstipation
Diagnosis & Test
The following laboratory studies and imaging test are helpful in the diagnostic treatment of bowel obstruction
- History and physical examination
- Full blood count (FBC)
- Hematocrit level estimation
- Prothrombin time (PT)
- Urinalysis
- Blood grouping and cross matching
- Stool guaiac test
- Abdominal x-ray
- Computed tomography (CT) scan with contrast
- Colonoscopy
- Ultrasound
- Magnetic Resonance Imaging
You may also like: Pathophysiology of Intussusception
Management of Bowel Obstruction
Management of intestinal obstruction is directed at correcting physiologic changes caused by the obstruction. Treatment depends on the Aetiology, site of obstruction, the extent of the progression of the condition and treatment option and expertise available. Conservative management is the first choice of treatment unless there are signs of intestinal perforation, ischemia and hernias. An appropriate intravenous fluid resuscitation is recommended. Pain relievers and antibiotics (to treat intestinal overgrowth of bacteria and translocation across the bowel wall) are administered. Patients with significant abdominal distention and vomiting, nasogastric tube is inserted to relieve discomfort and decompress the distended proximal bowel. Nil per Os is maintained. Anti-emetics and bowel rest is also considered. Urinary catheter may be inserted to monitor and obtain strict fluid balance
Surgical Management
The mainstay of surgical treatment demand for obstructions includes internal hernias, perforation or ischemia. Small bowel obstructions caused by tumors (adenocarcinoma, neuroendocrine tumors, lymphomas) are treated with resection and anastomosis. Large bowel obstructions caused by diverticular without perforation is treated with resection and primary anastomosis.
A right hemicolectomy with primary anastomosis is the choice of procedure for patient with right-sided LBO. In this procedure, the distal ileum is anastomosed to the proximal transverse colon after high ligation of the ileocolic vessel.
Hartmann's procedure is mostly performed for Left-sided LBO. There is surgical resection of the sigmoid colon and part of the upper rectum. Colonic stent and dilation is also used for both left and right-sided LBOs. LBO caused by sigmoid volvulus is treated by Endoscopic reduction or detorsion
Nursing management of Bowel Obstruction
- Assess patient usual pattern of bowel movement, sounds and note characteristics and frequency.
- Monitor patient laboratory studies; serum albumin, transferrin, WBC and RBC counts, serum electrolytes
- Administer Intravenous Fluids and electrolyte replacement as ordered
- Prepare and assist patient for Surgery if Indicated
- Provide Emotional Support and Patient Education prior to surgery
- Assess patient for pain and administer pain medications as ordered.
- Encourage patients to eat small, frequent meals as tolerated.
- Assess patient nutritional and dietary status
- Maintain patient NPO status as ordered.
- Assess patient nutritional and dietary status
- Weigh patient daily.
- Provide comfort measures.
- Monitor intake and output.
- Administer Medications as Prescribed
- Encourage use of relaxation techniques, deep-breathing exercises, etc.
- Educate patient on the importance of smoking cessation.
- Provide a warm sitz bath as appropriate for a patient experiencing constipation related to hemorrhoid or SBO to relieve pain and discomfort
- Patient Education on regular Follow-Up
Complications of Bowel Obstruction
- Short bowel syndrome
- Bowel perforation
- Intraabdominal abscess
- Sepsis
- Wound dehiscence
- Renal failure
- Death
Prevention of Bowel Obstruction
Preventing bowel obstruction, a person lifestyle can contribute to the condition as well as preventive measures, therefore lifestyle and diet modification is a key to prevention.
- Exercise regularly.
- Drink enough fluids or water to remain hydrated
- eat smaller meals throughout the day and chew thoroughly while eating
- Avoid foods high in fiber, raw fruits and vegetables, and fiber supplements.
Differential Diagnosis
- Gastroenteritis
- Chronic megacolon
- Diverticulitis
- Acute pancreatitis
- Bowel perforation
- Acute appendicitis
- Toxic megacolon
- Abdominal hernias
References
- Catena, F, De Simone, B, Coccolini, F, Di Saverio, S, Sartelli, M & Ansaloni, L 2019, ‘Bowel obstruction: A narrative review for all physicians’, World Journal of Emergency Surgery, vol. 14, no. 1.
- Chandra, R 2019, ‘Large bowel obstruction’, Textbook of Surgery, pp. 285–292.
- Elmisbah, HOII, Alonezy, AAM, Alanazi, STA & Alanazi, SNA 2022, ‘Intestinal Obstruction Etiology, Diagnosis and Management’, Journal of Pharmaceutical Research International, pp. 33–41.
- Family, A, Jackson, P & Raiji, M 2011, ‘Evaluation and Management of Intestinal Obstruction’, vol. 83, no. 2.
- Klingbeil, KD, Wu, JX, Osuna-Garcia, A & Livingston, EH 2022, ‘Management of small bowel obstruction and systematic review of treatment without nasogastric tube decompression’, Surgery Open Science, vol. 12.