
What to expect in this article
What is Appendicitis
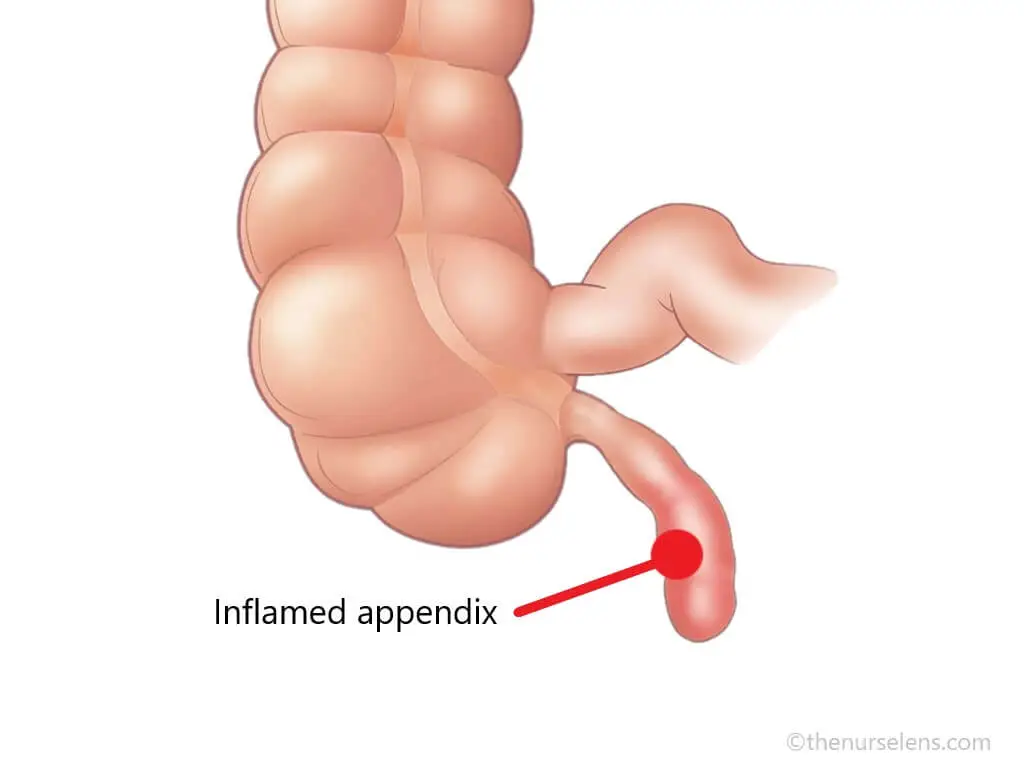
Inflamed Appendix: Appendicitis
Appendicitis is the inflammation of the appendix, a small, tube-like structure attached to the large intestine at its lower right end. The condition is one of the most frequent causes of acute to severe abdominal pain and can present in various forms, ranging from simple inflammation to complicated cases involving perforation or abscess formation. It is a common and potentially serious medical condition that often requires surgical intervention (appendectomy).
Incidence of Appendicitis
The incidence of appendicitis varies geographically and across age groups. The condition is most prevalent among individuals aged 10 to 30 years, although the overall incidence has been declining in recent decades
Causes of Appendicitis
The exact cause of appendicitis is not fully understood, but several factors contribute:
- Obstruction: Luminal Obstruction, (a small hole called lumen in the appendix) is a blockage in the appendix, often caused by fecaliths (hardened stool), lymphoid hyperplasia, foreign bodies, or tumors, leading to inflammation.
- Infections: Viral or bacterial infections can lead to blockage, swelling of the lymphoid tissue in the appendix, which may obstruct the appendix.
- Genetic Factors: A family history of appendicitis might increase one susceptibility to appendicitis.
- Age: Anyone can develop appendicitis, but it most often among individuals aged 10 to 30 years
- Gender: Women do have lower risk than men
Pathophysiology of Appendicitis
The presence of the lymphatic tissue in the appendix suggest a role in the immune system, however, its primary function is not clearly understood. In appendicitis, the primary pathogenic event is due to luminal obstruction which cause rise in both intramural and intraluminal pressure. This obstruction may result from a variety of causes, such as, lymphoid hyperplasia, fecaliths, foreign bodies, parasites, and by both primary and metastatic tumors. Increase in luminal pressure results in occlusion of small vessels, lymphatic stasis and thrombosis. The appendix become obstructed with vascular congestion and engorgement. As a result, ischemia and necrosis develops due to impaired vascular and lymphatic drainage. Bacteria (E-coli, Bacteroides, and Pseudomonas) overgrowth occurs progressing significant inflammation and necrosis. The appendix then becomes susceptible to perforation and burst leading to localized abscess. Peritonitis, may occur in severe cases.
Signs & Symptoms of Appendicitis
Recognizing the symptoms of appendicitis is crucial for timely treatment. Common clinical presentation of appendicitis typically includes:
- Abdominal Pain: Sudden pain that begins around the navel and migrating to the right lower quadrant (RLQ). The site of pain may vary, depending on individuality (age) and position of the appendix.
- Tenderness: Pain and tenderness to the touch in the lower right abdomen is a hallmark sign. This area may be sensitive to pressure (guarding) and elicit pain when pressure is released (rebound tenderness).
- Fever: Low-grade fever may be present, indicating inflammation.
- Loss of Appetite (Anorexia)
- Nausea and Vomiting
- Abdominal bloating
- Constipation or diarrhea with gas
Diagnostic Investigations & Test
Diagnosis of appendicitis is primarily clinical but may involve several investigations:
Laboratory Tests:A Full blood count (FBC) often shows leukocytosis (elevated white blood cell count) with a predominance of neutrophils.
Imaging Studies:Ultrasound (especially in children and pregnant women) and Computed Tomography (CT Scan, more sensitive and specific than ultrasound, CT scans can confirm the diagnosis by identifying an enlarged, non-compressible appendix) to visualize the inflamed appendix.
Urinalysis:Urine examination help rule out urinary tract infections (UTI’s) or kidney stones that may mimic symptoms of appendicitis.
Physical Examination:Healthcare provider will assess your symptoms and perform a physical exam. The characteristics and details of the abdominal pain are key feature to diagnosing appendicitis. Applying hand pressure to specific areas of the abdomen elicits different responses which guides the diagnosis. Some of the responses that indicate appendicitis may include;
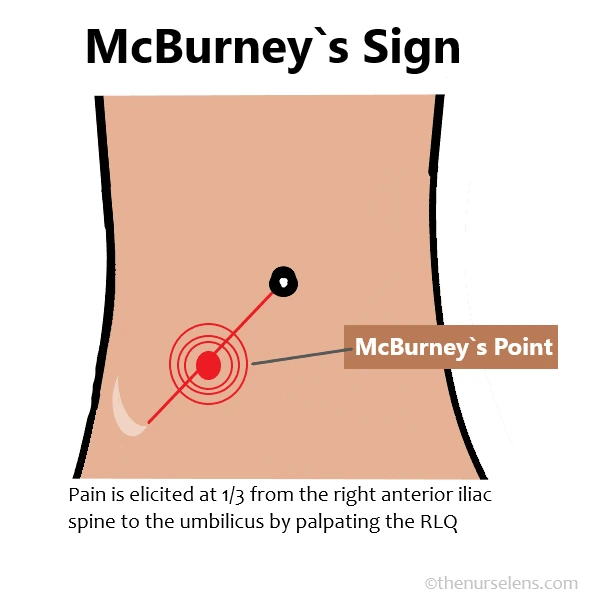
McBurney`s Point
- McBurney’s sign,also known as McBurney’s point tenderness is located one third of the distance from the right anterior superior iliac spine to the umbilicus (navel). This is when the patient pain is felt at this area, one-third from the right anterior iliac spine to the umbilicus, it indicates inflamed appendix
- Rovsing’s sign:This is pain felt at the right lower quadrant of the abdomen upon touching or palpating the left lower quadrant of the abdomen. Releasing the pressure elicit pain indicate the positive Rovsing`s sign and confirms appendicitis
- Psoas sign:Also known as Cope`s sign or Obraztsova's sign. The right psoas muscle runs over the pelvis near the appendix. Flexing the patient hip against resistance when lying supine will cause abdominal pain when the appendix is inflamed. To check for this, the patient is asked to lift the right thigh whiles lying down, if pain is felt in the RLQ, it indicate positive psoas sign
- The Obturator Sign:This is assessed when the patient is lying supine with the right leg bent at the knee. The healthcare provider passively flexes the hip and knee, then internally rotates the leg. If this maneuver causes pain in the right lower quadrant (RLQ), it indicates a positive obturator sign. This sign is significant because the right obturator muscle runs near the appendix, and moving the bent knee left and right requires flexing the obturator muscle, which can lead to abdominal pain if the appendix is inflamed
- Guarding:Guarding occurs when the patient involuntarily tenses the abdominal muscles during abdominal palpation.
- Rebound tenderness is when the patient pain temporarily worsens after sudden release of pressure or palpation of the right lower quadrant.
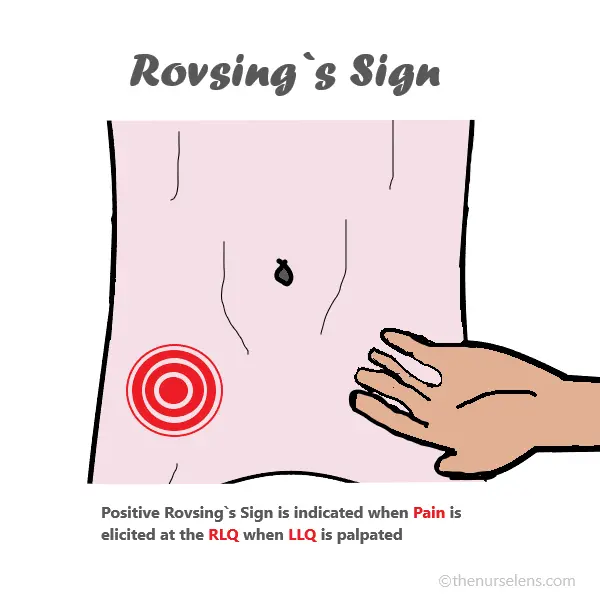
Positive Rovsing’s Sign
You may also like: Everything you need to know about Peptic Ulcer Disease
Treatment of Appendicitis
Appendicitis is treated as an emergency after diagnosed to avoid been rupture and prevent complications. The gold-standard treatment of appendicitis primarily involves surgical intervention, which can be performed through appendectomy
Appendectomy,which is the standard treatment, can be performed via open surgery or Laparoscopic techniques. Open surgery involves larger opening into the abdomen to remove the appendix, especially when ruptured. Laparoscopic surgery is a minimal invasive technique using smaller incisions. Laparoscopic surgery is associated with shorter recovery times and less postoperative pain which is preferred over open approach for most uncomplicated appendicitis.
Non-Operative Management:In some cases of uncomplicated appendicitis, non-operative management with antibiotics may be considered, especially for patients who are not surgical candidates. A combination of antibiotic is used after culture and sensitivity results to treat both aerobic and anaerobic bacteria. A third-generation cephalosporin, such as ceftriaxone, or a beta-lactamase inhibitor, such as ampicillin-sulbactam, is used against aerobic gram-negative bacteria. Whiles either metronidazole or clindamycin is used against anaerobic bacteria.
Nursing Management of Appendicitis
The following are the measures to put in place in the care of patient's with Appendicitis
Pre-operative management
- Check and monitor patient vital signs
- Reduce the anxiety level of patient by keeping the patient informed of the plan of care and treatment options.
- Monitor for changes in patient level of pain.
- Maintain an NPO status.
- Administer fluid and electrolyte intravenously as prescribed to prevent dehydration and correct electrolyte imbalance.
- Obtain and monitor laboratory values, particularly the white blood cell count, as an increase can signal infection.
- Monitor for signs of a ruptured appendix and peritonitis.
- Administer antibiotics as prescribed.
- Avoid the use of pain medications so as not to mask pain changes associated with perforation.
- Monitor bowel sounds.
- Teach and encourage non-pharmacological pain management techniques such as deep breathing and relaxation exercises.
- Position patient in a right side-lying to semi Fowler's position to promote comfort
- Apply ice pack to the abdomen for 20 to 30 minutes every hour if prescribed.
- Avoid laxative or enema
Post-operative management
- Monitor vital signs, particularly the temperature.
- Maintain an NPO status until bowel function has returned
- Assess the incision site for signs of infection, such as redness, swelling, drainage, and pain.
- Monitor Penrose drain drainage, if inserted, as prescribed.
- Regularly change the dressing as prescribed, and record the type and amount of drainage.
- Perform wound irrigations if prescribed.
- Maintain an aseptic technique during any invasive procedures or wound care.
- Monitor for adequate bowel movements.
- Maintain accurate intake and output records
- Encourage oral fluid intake when appropriate and as tolerated.
- Maintain nasogastric tube suction and patency of the tube if present.
- Encourage and assist patient to walk as can tolerate or permitted to maintain circulation
- Administer antibiotics and analgesic as prescribed.
Complications of Appendicitis
Untreated or delayed treatment of appendicitis can quickly lead to very serious complications, which is why it is treat it as an emergency. Complications of appendicitis include
- Perforation: The appendix can rupture, causing infection in the abdominal cavity (peritonitis). It can also spread to the bloodstream leading to septicemia which can be fatal.
- Abscess Formation: A localized collection of pus can form around the appendix.
- Postoperative Infections: Infections at the surgical site or within the abdomen can occur and has been the most common complication. These may include wound infections, intra-abdominal abscesses, and ileus, with varying rates between open and laparoscopic surgeries
Preventions of Appendicitis
While there is no guaranteed way to prevent appendicitis, certain strategies may help reduce the risk:
- While there is no guaranteed way to prevent appendicitis, some strategies that may help reduce the risk include:
- Maintaining a diet rich in high-fiber to prevent constipation and fecalith formation
- Seeking prompt medical care immediately If you experience any of the above symptoms, can prevent complications
- Early recognition and treatment of abdominal pain can prevent complications associated with delayed diagnosis
Differential Diagnosis of Acute Appendicitis
- Gastroenteritis
- Endometriosis
- Pelvic Inflammatory Disease
- Renal Colic
- Kidney Stones
- Irritable Bowel Disease
- Mesenteric Adenitis
- Ruptured Ovarian Cyst
- Ectopic Pregnancy
- Testicular Torsion
References
- Acute appendicitis – PMC: https://pmc.ncbi.nlm.nih.gov/articles/ PMC1562475/
- Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines | World Journal of Emergency Surgery
- Lotfollahzadeh S, Lopez RA, Deppen JG. Appendicitis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan
